
Why Cancer Screening Is About Timing, Not Fear
Cancer screening is the process of checking for certain cancers before symptoms appear. It is not the same as diagnosing cancer in a person who already has warning signs. Screening is used to identify disease early in selected groups of people or to find precancerous changes that may be treated before they become more serious. This is why cancer screening guidelines by age matter: the right test at the right time can be more useful than testing too early, too late, or without a clear reason.
Many adults delay screening because they feel healthy, fear the result, do not know which test applies to them, or assume that cancer always causes obvious symptoms. In reality, several screening programs are designed specifically for people without symptoms. The Centers for Disease Control and Prevention explains that screening means checking the body for cancer before symptoms are present, and that regular screening may help find breast, cervical, colorectal, and lung cancers early, when treatment is more likely to work well.
The goal of screening is not to create anxiety or test every person for every cancer; the goal is to match the right patient with the right screening discussion based on age, risk factors, sex, family history, and prior results.
Screening recommendations are built around evidence. A screening test should offer enough benefit for a specific group of people to justify possible downsides, including false positives, false negatives, overdiagnosis, anxiety, follow-up procedures, radiation exposure in some tests, cost, and unnecessary treatment. This is why guidelines can differ by age group, risk level, and medical organization.
A patient may ask why screening does not begin for every cancer at age 18 or why a scan is not recommended every year “just to be safe.” The answer is that more testing is not always better. A useful screening test must find disease early enough to improve outcomes and must be accurate enough to avoid creating more harm than benefit in people who are unlikely to have the disease.
At the same time, avoiding screening completely can be risky. Some cancers may not cause symptoms until they are more advanced. Colorectal cancer, breast cancer, cervical cancer, and lung cancer in high-risk patients are examples where organized screening can play an important role. A physician helps the patient understand which tests are relevant now, which may be needed later, and which are not appropriate based on the current situation.
Routine primary care often becomes the starting point for these conversations. During a preventive visit, a physician can review age, sex, smoking history, family history, previous abnormal findings, symptoms, and past screening records. Patients who are not sure where to begin may benefit from first reviewing annual check-ups that help organize preventive care.
It is also important to separate screening from diagnostic evaluation. If a patient has a breast lump, blood in the stool, coughing blood, unexplained weight loss, abnormal bleeding, persistent pain, or another concerning symptom, that is not simply a routine screening question. Symptoms may require diagnostic testing, imaging, laboratory work, or specialist evaluation. Screening is for people who meet criteria before symptoms appear; symptoms require individualized medical assessment.
Because recommendations can change, patients should not rely only on memory or advice from years ago. For example, major organizations periodically update guidance for breast, colorectal, cervical, lung, and prostate cancer screening as evidence evolves. The American Cancer Society updated its cancer screening guidance page in December 2025, while the U.S. Preventive Services Task Force updated its breast cancer screening recommendation in April 2024. A physician can help patients apply current guidance to their personal risk profile.
How Doctors Decide Which Screenings You Need
A cancer screening recommendations discussion usually begins with risk. Age is important, but it is not the only factor. Two patients of the same age may need different conversations if one has a strong family history, a previous abnormal result, a history of smoking, a genetic syndrome, immune suppression, or symptoms that require diagnostic evaluation rather than routine screening.
The first factor is age. Many screening recommendations are organized around the ages when the balance of benefit and harm becomes more favorable for average-risk adults. This is why colorectal cancer screening is commonly discussed beginning in midlife, while cervical cancer screening begins earlier, and lung cancer screening is limited to people with specific smoking-related risk. Age helps structure the conversation, but it does not replace individual judgment.
Sex and organs at risk also matter. Breast, cervical, prostate, and certain gynecologic cancer screening discussions depend on anatomy, medical history, prior surgeries, hormone-related factors, and personal risk. Patients who have had hysterectomy, mastectomy, prostate surgery, gender-affirming surgery, or complex medical history should not assume general charts apply to them without physician review.
Family history can change timing. A close relative with colorectal cancer, breast cancer, ovarian cancer, pancreatic cancer, prostate cancer, or other inherited cancer patterns may lead a physician to discuss earlier screening, genetic counseling, or specialist referral. The age at which the relative was diagnosed is often important. A parent diagnosed at 82 may influence risk differently than a sibling diagnosed at 42.
Previous abnormal results also change the plan. A patient who had an abnormal Pap test, colon polyp, abnormal mammogram, suspicious lung finding, or previous biopsy may need surveillance rather than routine average-risk screening. Surveillance is more individualized and usually follows a specific plan based on the prior result.
Smoking history is central to lung cancer screening decisions. Lung screening is not recommended for every adult. It is generally reserved for people at higher risk because of smoking exposure and age range, using low-dose CT when criteria are met. The American Cancer Society and USPSTF both support lung cancer screening for selected higher-risk adults, but details may differ, and insurance coverage may depend on the guideline used.
General health and life expectancy also influence screening. Screening is most useful when a patient is healthy enough to benefit from early detection and follow-up treatment if needed. In older adults or people with serious illness, the decision may shift from routine screening to individualized discussion about benefits, burdens, and patient goals.
Factors Your Physician May Review Before Recommending Screening
A screening plan is more accurate when your physician can evaluate several parts of your health history together:
- Your current age and previous screening history
- Personal history of cancer, polyps or abnormal results
- Family history and age of diagnosis in close relatives
- Smoking history or other exposure-related risks
- Symptoms that may require diagnostic evaluation
- Prior surgeries or anatomy-related considerations
- Medication use, immune status and chronic conditions
- Your ability and willingness to complete follow-up testing
A screening plan is only useful if the patient understands it and can complete the next step. Some tests require preparation, some require repeat intervals, and some require follow-up if the result is abnormal. A physician should explain not only which test is recommended, but also what happens if the result is positive, unclear, incomplete, or abnormal.
Common Adult Screenings to Discuss by Age Group
The table below is a general patient-education overview, not a personal medical schedule. Specific recommendations may differ depending on country, medical organization, personal risk, symptoms, prior results, and insurance rules. Patients should use it as a starting point for discussion with a clinician.
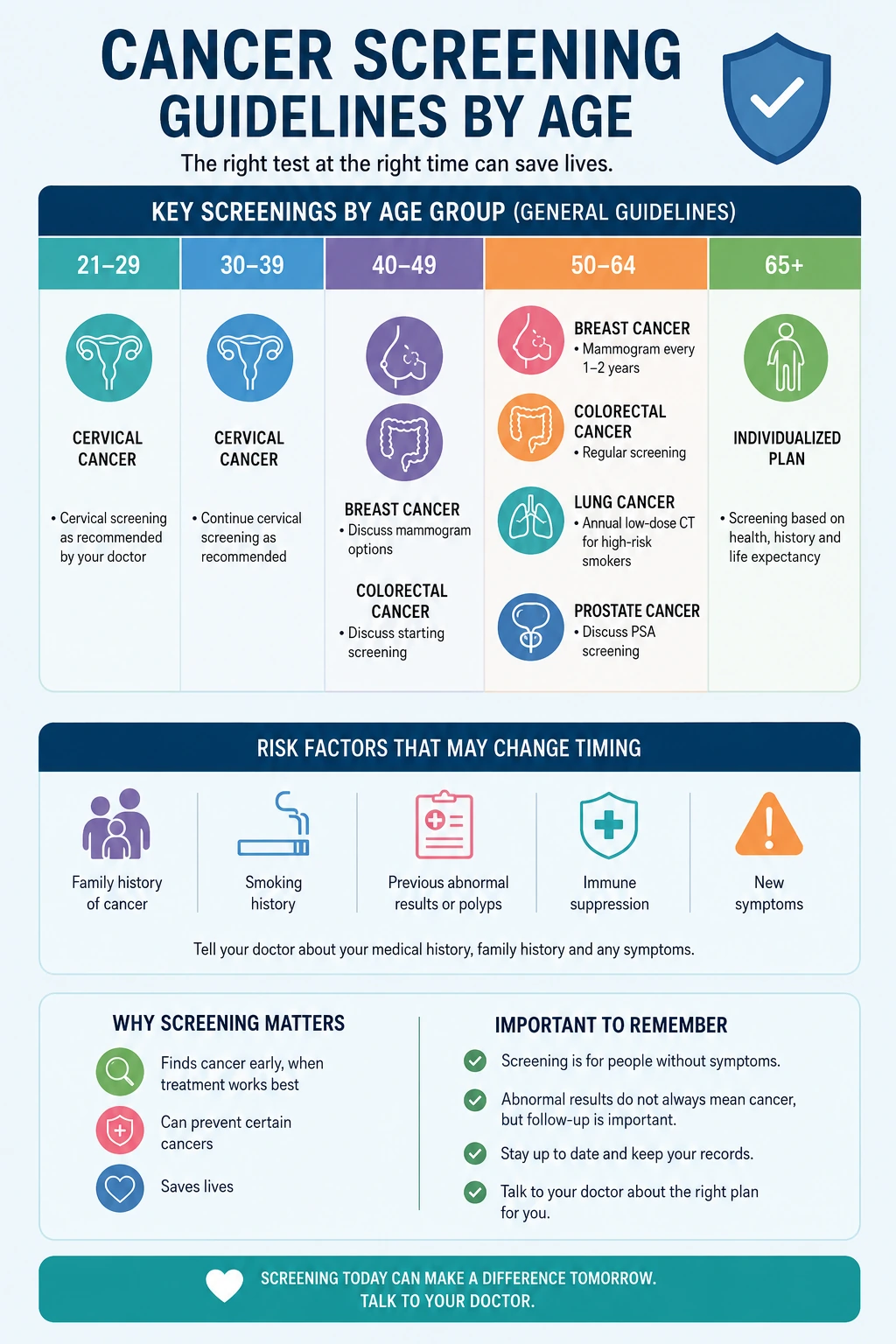
| Age range | Screenings to discuss | Risk factors that may change timing | Follow-up considerations |
|---|---|---|---|
| 21–29 | Cervical health screening when applicable | Prior abnormal results, immune status or specific medical history | Follow the interval recommended by the clinician |
| 30–39 | Cervical health screening and risk-based discussions | Family history, symptoms or previous abnormal findings | Keep records of previous tests and results |
| 40–49 | Breast screening discussion, colorectal screening discussion near midlife, risk-based review | Family history, genetic risk, prior abnormal results or symptoms | Clarify when to begin and which method is appropriate |
| 50–64 | Breast, colorectal, cervical, prostate and lung screening discussions when relevant | Smoking history, anatomy, family history, prior polyps or abnormal imaging | Abnormal results may require imaging, colonoscopy, biopsy or specialist care |
| 65–75 | Colorectal, breast, lung, cervical or prostate-related discussions depending on history | Previous screening history, overall health and risk level | Some screenings may continue, stop or become individualized |
| Over 75 | Individualized discussion based on health status and prior results | Life expectancy, treatment goals, prior abnormal results or new symptoms | Benefits and burdens should be reviewed with the physician |
This type of overview helps adults see that adult cancer screening is not one single test. It is a series of age- and risk-based decisions. A person may be current on one screening and overdue for another. Another patient may not need a test yet but should know when to start the conversation.
Documentation matters. Patients should keep track of previous screening dates, results, recommendations, and follow-up instructions. This is especially important after a move, insurance change, hospital visit, or specialist referral. Missing records can lead to unnecessary repeat testing or missed follow-up.
Breast, Cervical and Women’s Cancer Screening
Breast and cervical screening are two of the most familiar cancer prevention topics, but many patients are still uncertain about timing, intervals, and what results mean. Recommendations can vary by organization, risk level, and prior findings. The safest approach is to review screening history with a clinician and make sure the plan fits the patient’s age and risk factors.
For breast cancer screening, the USPSTF recommends that women receive screening mammography every other year from age 40 through 74. This recommendation applies to women at average risk and is designed to reduce the risk of dying from breast cancer. Patients with a strong family history, genetic risk, prior chest radiation, previous abnormal imaging, or other high-risk factors may need a different plan.
Mammography can be used as a screening tool when no symptoms are present, but breast symptoms require diagnostic evaluation. A new lump, nipple discharge, skin dimpling, persistent focal pain, redness, swelling, or other breast change should not wait for a routine screening appointment. The clinician may recommend diagnostic mammography, ultrasound, MRI in selected cases, or referral depending on the finding.
Cervical cancer screening is usually based on age, HPV-related risk, previous Pap or HPV test results, immune status, and history of cervical procedures. Patients should not assume they are finished with screening because symptoms are absent. Cervical precancerous changes may not cause symptoms early, which is why regular screening has a preventive role.
Women’s health screening is not limited to cancer. A visit may also include blood pressure, metabolic risk, bone health, menstrual changes, menopause symptoms, sexual health, pelvic symptoms, family history, sleep, mood, and medication review. Patients who want a broader checklist can review screenings every woman should schedule this year.
Imaging services may also become part of women’s screening or follow-up care. Mammography is the most common example, but ultrasound or MRI may be considered in selected situations. Imaging should be chosen based on the clinical question, not simply on the idea that more testing is always better. A separate guide on mammography and other imaging used in early detection can help patients understand why different tests are used for different reasons.
Colorectal Cancer Screening: Why Many Adults Delay It
Colorectal screening is one of the most important prevention conversations for adults in midlife and later adulthood, yet many patients postpone it. Some delay because they feel well. Others worry about preparation, embarrassment, discomfort, cost, time off work, or what the result might show. These concerns are common, but avoiding the conversation can mean missing the chance to find a problem earlier.
The USPSTF recommends screening for colorectal cancer in all adults ages 45 to 75. For adults ages 76 to 85, the decision is individualized and should consider overall health, previous screening history, and patient preferences. This age-based approach is important because the value of screening depends on both cancer risk and whether the patient is likely to benefit from detection and follow-up.
Colorectal screening can involve different methods, including stool-based tests and direct visualization tests such as colonoscopy. These options are not identical. Some are done more frequently, some require bowel preparation, some can be completed at home, and some allow removal of polyps during the procedure. The right choice depends on the patient’s risk, preferences, medical history, test availability, and ability to complete follow-up if the result is abnormal.
A common mistake is assuming that screening is unnecessary without symptoms. Blood in the stool, unexplained weight loss, persistent change in bowel habits, anemia, abdominal pain, or weakness should be discussed with a physician, but screening is designed to evaluate eligible patients before these signs appear. Waiting for symptoms can reduce the preventive value of the test.
Another mistake is completing a stool-based test but not following up after an abnormal result. Stool tests can be useful when selected appropriately, but an abnormal result usually requires additional evaluation. Patients should ask their clinician what the next step would be before choosing a screening method, so they understand the full process.
Family history can also change the plan. A patient with a close relative diagnosed with colorectal cancer or advanced polyps, especially at a younger age, may need earlier or different screening. Patients should tell their physician the type of cancer, which relative was affected, and the age at diagnosis if known.
Lung Cancer Screening for Higher-Risk Patients
Lung cancer screening is different from many other screening conversations because it is not intended for the general adult population. It is reserved for people with higher risk based mainly on age and smoking history. The usual test is low-dose computed tomography, which can detect lung findings earlier than symptoms in selected patients, but it also has limitations and possible harms.
The USPSTF recommends annual lung cancer screening with low-dose CT for adults ages 50 to 80 who have a 20 pack-year smoking history and currently smoke or have quit within the past 15 years. Screening should stop once a person has not smoked for 15 years or develops a health problem that substantially limits life expectancy or the ability or willingness to have curative lung surgery.
Patients should not order lung imaging for screening without a clinician’s guidance. Eligibility matters because low-dose CT can find nodules that are not cancer, leading to repeat imaging, anxiety, additional tests, or procedures. On the other hand, eligible higher-risk patients may benefit from a structured screening program that includes counseling, follow-up plans, and smoking cessation support when relevant.
Smoking history should be discussed honestly and specifically. Pack-year calculation depends on how much a person smoked and for how long. For example, one pack per day for 20 years equals 20 pack-years, while two packs per day for 10 years also equals 20 pack-years. The physician can calculate this and decide whether screening criteria are met.
Lung symptoms should be handled differently from screening. Coughing blood, unexplained weight loss, persistent chest pain, worsening shortness of breath, or a cough that does not improve may require diagnostic evaluation regardless of whether the patient meets screening criteria. Screening guidance applies to eligible people without symptoms; symptoms require individualized care.
Because lung screening uses CT imaging, patients may also want to understand how imaging fits into prevention and diagnosis. CT imaging used for certain screening decisions can help explain why different imaging tests are used for different clinical questions.
Prostate Cancer Screening: A Shared Decision
Prostate cancer screening is a good example of why screening decisions are not always automatic. The potential benefits and harms should be discussed with a clinician, especially because screening can lead to follow-up testing, biopsy, diagnosis of slow-growing disease, treatment side effects, or anxiety. At the same time, some patients have higher risk and may reasonably want a more detailed conversation.
The USPSTF states that for men ages 55 to 69, the decision to undergo periodic prostate-specific antigen screening should be individualized after discussing potential benefits and harms with a clinician. For men age 70 and older, the USPSTF recommends against PSA-based screening. These recommendations apply to screening decisions, not to evaluation of symptoms.
Symptoms such as difficulty urinating, blood in the urine, pelvic pain, bone pain, unexplained weight loss, or other concerning changes should be evaluated medically. Symptoms do not automatically mean cancer, but they should not be managed as a routine screening question. A physician can decide whether PSA testing, urine testing, imaging, urology referral, or another evaluation is appropriate.
Risk can vary. Family history, Black ancestry, known genetic variants, prior PSA results, age, general health, and patient preferences may influence the conversation. The patient should ask what a positive result would mean, what follow-up might involve, and how the physician weighs the chance of benefit against possible harm.
Shared decision-making is especially important because different patients value trade-offs differently. One patient may prioritize early detection even with the possibility of unnecessary follow-up. Another may prioritize avoiding testing that could lead to procedures for a cancer that may never cause harm. The clinician’s role is to explain the evidence clearly, not pressure the patient into a one-size-fits-all choice.
What Happens After an Abnormal Screening Result
An abnormal screening result can be frightening, but it does not always mean cancer. Screening tests are designed to identify findings that may need a closer look. Sometimes the next step confirms that there is no cancer. Sometimes it identifies a precancerous change, benign condition, early cancer, or finding that needs monitoring. The meaning depends on the test, the result, and the patient’s history.
After an abnormal result, the physician may recommend repeat testing, diagnostic imaging, laboratory work, specialist referral, biopsy, colonoscopy, additional views, ultrasound, MRI, CT, or close follow-up. The next step should be specific. Patients should ask what the result means, how urgent the follow-up is, what test is recommended next, and what would happen depending on the next result.
For breast screening, an abnormal mammogram may lead to additional mammographic views, ultrasound, MRI in selected cases, or biopsy. Many callbacks do not result in a cancer diagnosis, but follow-up is still important because the purpose is to clarify the finding.
For colorectal screening, an abnormal stool-based test often leads to colonoscopy. During colonoscopy, a clinician may examine the colon and remove certain polyps if found. Follow-up intervals depend on the findings, pathology results, number and type of polyps, quality of the exam, and patient risk factors.
For cervical screening, abnormal results may lead to repeat testing, HPV-related follow-up, colposcopy, or other evaluation based on the result and age. The purpose is often to identify and manage precancerous changes before they progress.
For lung screening, a finding on low-dose CT may lead to repeat imaging after a defined interval, specialist review, PET imaging, biopsy, or other testing depending on size, appearance, growth, and patient risk. Not every lung nodule is cancer, but organized follow-up is essential.
Laboratory and imaging services often support this follow-up process. Lab teams may process pathology, blood work, or other specimens, while imaging teams help clarify findings seen on screening or physical exam. Patients can learn more about how laboratory services support diagnostic decisions and imaging tests that help clarify findings.
An abnormal screening result is not a final diagnosis; it is a signal that the care team needs to complete the next appropriate step before drawing conclusions.
Risk Factors That May Change Screening Timing
Average-risk guidelines are useful, but they do not apply perfectly to every patient. Some adults need earlier screening, different methods, shorter follow-up intervals, or specialist input because their risk is higher than average. Others may need screening to stop or become more individualized because age, health status, or previous results change the balance of benefit and harm.
| Risk factor | Why it may matter | What to discuss with a physician |
|---|---|---|
| Close relative with cancer at a young age | May suggest inherited or family-related risk | Whether earlier screening or genetic counseling is appropriate |
| Previous abnormal screening result | May require surveillance rather than average-risk screening | Recommended interval and next test based on the prior finding |
| History of polyps | May change follow-up timing after colon evaluation | Type, number and pathology of previous findings |
| Smoking history | May affect lung screening eligibility | Pack-year calculation and years since quitting |
| Immune suppression | May increase risk for certain infections and cancers | Whether screening intervals or methods should be adjusted |
| New symptoms | May shift the question from screening to diagnosis | Which evaluation is needed now rather than later |
Patients should update their physician when family history changes. New diagnoses in parents, siblings, children, grandparents, aunts, uncles, or cousins may be relevant depending on the cancer type and age at diagnosis. It can also help to ask relatives about exact diagnoses rather than using broad terms such as “stomach cancer” or “female cancer,” because screening implications may differ.
Patients should also report prior abnormal findings even if they happened years ago. A colon polyp, abnormal Pap test, breast biopsy, lung nodule, or genetic test result may affect future planning. If records are not available, the physician may help request them or decide the safest next step based on available information.
How to Prepare for a Screening Appointment
A screening appointment is more useful when the patient arrives with accurate information. Many recommendations depend on details that are easy to forget during the visit, especially dates of previous tests, abnormal results, family history, smoking history, surgeries, and symptoms. Preparation helps the physician decide whether the patient needs routine screening, diagnostic evaluation, specialist referral, or no test at that time.
Patients should bring records of previous screenings whenever possible. This may include mammogram reports, colonoscopy reports, pathology results, Pap or HPV test results, CT reports, prostate-related test results, biopsy reports, genetic testing results, or letters from specialists. If exact records are not available, approximate dates and the name of the facility can still help.
Family history should be specific. The physician may need to know which relative had cancer, what type of cancer it was, and the age at diagnosis. A vague statement such as “cancer runs in my family” is less useful than knowing that a parent had colorectal cancer at 48 or a sister had breast cancer at 42. These details can change the timing and type of screening discussion.
Patients should also mention symptoms, even if the appointment was scheduled for routine screening. Blood in the stool, unexplained weight loss, a new breast lump, abnormal bleeding, persistent cough, coughing blood, worsening pain, change in bowel habits, or difficulty urinating may shift the visit from screening to diagnostic evaluation. That does not mean cancer is present, but it means the physician should not treat the concern as routine.
Smoking history should be described clearly. For lung screening, the physician may calculate pack-years based on how many packs per day the person smoked and how many years they smoked. Patients should also mention when they quit, whether they currently smoke, and whether they need support with quitting.
What to Bring or Know Before the Visit
A prepared patient can help the care team build a more accurate plan:
- Dates and results of previous screening tests
- Reports from colonoscopy, mammography, CT, Pap, HPV or biopsy results
- Family history, including cancer type and age at diagnosis
- Smoking history and quit date if relevant
- Any new symptoms or changes from your usual health
- Prior surgeries or anatomy-related medical history
- Current medications and immune system-related conditions
- Questions about benefits, risks and follow-up steps
It is also reasonable to ask what happens after each possible result. A patient should understand what a normal result means, what an abnormal result may require, how quickly follow-up should happen, and when the next screening should be discussed. Screening is a process, not a single isolated appointment.
How Screening Fits Into a Long-Term Prevention Plan
Preventive cancer screening works best when it is part of a broader health plan. It should be coordinated with primary care, women’s health, imaging, laboratory services, smoking cessation, chronic disease management, and age-based prevention. A patient who completes one screening but skips routine follow-up may still miss other important risks.
Primary care often coordinates this process. During a routine visit, a physician can check which screenings are current, which are due, which can wait, and which require specialist input. This is especially useful for adults who receive care from multiple clinics or who have moved, changed insurance, or had tests performed at different facilities.
Women’s health care may focus on breast, cervical, pelvic, hormonal, bone, and reproductive health concerns, but it also connects with broader prevention. Blood pressure, diabetes risk, sleep, weight, mental health, family history, and medication review can all influence long-term health. For many patients, a women’s health checklist helps organize which topics should be discussed during the year.
Imaging services support screening and follow-up when clinically appropriate. Mammography, low-dose CT, ultrasound, MRI, and diagnostic imaging have different roles. Patients should not assume that one test is better for every situation. The best test is the one that fits the clinical question, risk level, symptoms, and guideline-based recommendation.
Laboratory and pathology services may also be involved, especially after biopsies, abnormal findings, or certain follow-up evaluations. The patient may never meet every person involved in processing results, but the quality and coordination of the diagnostic process matter. Clear communication between the ordering physician, laboratory, imaging team, specialists, and patient helps avoid delays and confusion.
Lifestyle and prevention should also be part of the conversation. Screening can help detect certain cancers earlier, but it does not replace smoking cessation, vaccination when appropriate, healthy weight support, physical activity, alcohol moderation, sun protection, and management of chronic disease. A physician can help patients focus on the most relevant prevention steps rather than trying to change everything at once.
Patients should also understand that screening plans may change. A new family diagnosis, abnormal result, new symptom, updated guideline, change in health status, or new medication may require the plan to be reviewed. This is why screening should be revisited periodically rather than treated as a one-time decision.
When Screening Is Not the Same as Diagnosis
One of the most important distinctions in cancer care is the difference between screening and diagnosis. Screening is performed in people who meet criteria and do not have symptoms of the disease being screened for. Diagnosis is performed when a patient has a symptom, abnormal exam finding, abnormal screening result, or other reason to investigate a possible disease.
This distinction changes the urgency and type of testing. For example, a routine mammogram for an average-risk woman is different from diagnostic breast imaging for a new lump. A stool-based colorectal screening test is different from evaluating blood in the stool. A low-dose CT for lung screening is different from investigating coughing blood or unexplained weight loss.
Patients should not wait for a screening appointment when they have concerning symptoms. Symptoms need medical evaluation, even if the patient is not yet in the usual screening age range. Cancer is not the only possible explanation for these symptoms, but the presence of symptoms changes the clinical question.
At the same time, patients should not panic if a physician recommends diagnostic follow-up. Diagnostic testing means more information is needed. It does not automatically mean cancer is present. It means the care team is moving from a broad screening question to a more specific evaluation.
The best next step depends on the symptom, the test result, and the patient’s risk. A physician may recommend imaging, laboratory testing, endoscopy, biopsy, specialist referral, repeat testing, or watchful follow-up with a defined timeline. Patients should ask what the purpose of the next test is and what results would change the plan.
Medical Disclaimer
This article is for educational purposes only and does not replace professional medical advice, diagnosis, or treatment. Screening recommendations vary by country, guideline, age, risk factors, symptoms, and personal medical history; speak with a qualified clinician about the right plan for your situation.
Author
By Dr. Cody R. Christensen, M.D. He practices at Sweetwater Medical Center, where he integrates pharmacologic treatment with lifestyle medicine and psychotherapy to support lasting patient wellness.
Medically Reviewed: by Clinical Pharmacy Board
Last Updated: 08.06.2026
FAQ
At what age should adults start cancer screening?
The starting age depends on the type of cancer, personal risk, family history, sex, anatomy, and prior results. Many adults should begin discussing several screenings in midlife, while some tests begin earlier or are limited to higher-risk patients.
Do I need screening if I have no symptoms?
Yes, screening is specifically designed for certain people before symptoms appear. Eligibility depends on age, risk factors, and the type of screening being considered.
Are cancer screening tests painful?
Some tests are quick and minimally uncomfortable, while others require preparation or a procedure. Your physician can explain what to expect and whether another screening option is appropriate for your situation.
What if my family has a history of cancer?
Tell your physician which relatives were affected, what type of cancer they had, and the age at diagnosis. This information may change the timing, method, or frequency of screening.
Does an abnormal result always mean cancer?
No. An abnormal screening result means additional evaluation may be needed. Many abnormal findings turn out to be benign, unclear, precancerous, or unrelated to cancer, but follow-up is still important.