
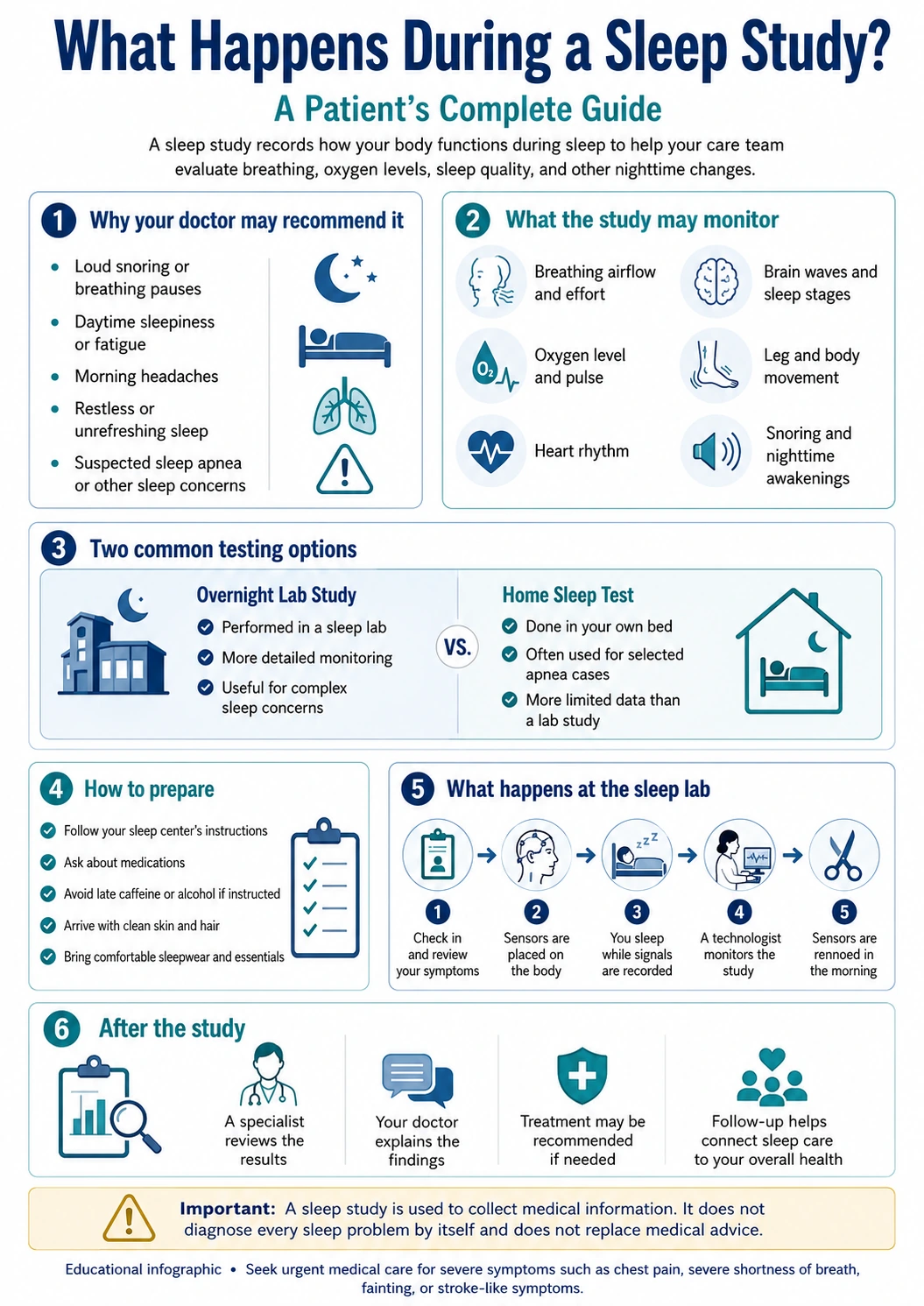
Why Your Doctor May Recommend a Sleep Study
A sleep study is a diagnostic test that records how your body functions while you sleep or try to sleep. It may be recommended when a physician suspects that poor sleep is not just a lifestyle problem, but a medical issue affecting breathing, oxygen levels, heart rhythm, daytime energy, mood, concentration, or long-term health. For many patients, the test is most closely associated with sleep apnea, but it can also help evaluate other sleep-related concerns depending on the clinical situation.
Many adults do not seek medical help for sleep symptoms because they assume snoring, waking up tired, or struggling to fall asleep is normal. Some patients blame work stress, aging, weight gain, late meals, screen time, or a busy schedule. These factors can matter, but they do not rule out a sleep disorder. When symptoms are frequent, disruptive, or linked to other medical risks, a structured evaluation may be more useful than guessing.
A sleep study is not ordered simply because someone had one bad night of sleep; it is usually considered when symptoms, risk factors, or medical history suggest that sleep quality, breathing, oxygen levels, or nighttime body functions need objective measurement.
One common reason for referral is loud, persistent snoring, especially when a bed partner notices pauses in breathing, choking, gasping, or restless movement during the night. A patient may not remember these episodes because they occur during sleep. Instead, the person may wake with dry mouth, morning headaches, fatigue, irritability, difficulty concentrating, or a feeling that sleep was not refreshing.
Another reason is excessive daytime sleepiness. Patients may fall asleep while reading, watching television, sitting in meetings, riding as a passenger, or in more dangerous situations such as driving. Daytime sleepiness can affect work performance, safety, mood, memory, and quality of life. It may also be misunderstood as laziness, depression, burnout, or poor discipline when the underlying issue is disrupted sleep.
A physician may also consider testing when sleep problems appear alongside other health concerns. High blood pressure, difficult-to-control blood pressure, heart rhythm concerns, obesity, diabetes risk, morning headaches, or repeated nighttime awakenings can make sleep evaluation more important. Patients with elevated blood pressure may also benefit from reviewing blood pressure warning signs that may need medical attention.
Insomnia can also lead to evaluation, but the reason matters. Not every patient with insomnia needs overnight testing. If the main issue is difficulty falling asleep because of stress, schedule, anxiety, medications, caffeine, or poor sleep habits, the physician may begin with a clinical assessment and behavioral recommendations. However, when insomnia is mixed with snoring, breathing pauses, leg movements, frequent awakenings, unusual behaviors during sleep, or major daytime impairment, further testing may be appropriate.
Some patients are referred after a partner or family member notices symptoms. This can be important because many sleep disorders are more visible to others than to the patient. A person may insist that they sleep through the night, while someone nearby observes loud snoring, pauses in breathing, kicking movements, or repeated arousals. Bringing that outside observation to the appointment can help the physician decide whether testing is necessary.
A sleep evaluation can also support long-term preventive care. Poor sleep may affect blood pressure, weight management, mood, metabolism, and cardiovascular risk. It may also interfere with a patient’s ability to follow other health recommendations. This is why sleep symptoms are worth mentioning during routine care, even when the appointment is not specifically about sleep. A broader guide to preventive care visits that help coordinate long-term health can help patients understand where sleep fits into primary care.
What a Sleep Study Measures While You Rest
A sleep study does not judge whether a person “slept well” based only on how rested they feel in the morning. It records body signals that help trained professionals understand sleep structure, breathing patterns, oxygen levels, movement, and other nighttime changes. The exact setup depends on the type of study and the reason for testing.
In an overnight lab study, sensors may be placed on the scalp, face, chest, abdomen, legs, and finger. These sensors do not treat the problem and do not deliver painful stimulation. Their role is to record information. The care team uses this information to identify patterns that are difficult or impossible to measure from a patient’s memory alone.
Brain wave monitoring helps identify sleep stages and awakenings. This matters because a patient may spend enough hours in bed but still experience fragmented sleep. Breathing sensors can show airflow changes, pauses, shallow breathing, or irregular breathing patterns. Belts around the chest and abdomen may help measure breathing effort. A finger sensor may record oxygen saturation and pulse. Leg sensors may help identify movements that interrupt sleep.
Heart rhythm and heart rate may also be monitored during certain studies. Sleep disorders can be associated with changes in oxygen levels, arousals, and stress responses that may affect cardiovascular function during the night. This does not mean every patient with a sleep problem has a heart condition, but it explains why sleep information can be medically relevant beyond tiredness.
Video and audio monitoring may be used in a sleep lab to help interpret movements, snoring, body position, or unusual behaviors. Patients sometimes worry that this makes the test uncomfortable or invasive. In practice, the purpose is clinical documentation. It helps the sleep team match recorded signals with what was happening physically at the time.
What May Be Monitored During the Night
The details vary by test type and physician order, but an overnight study may record several kinds of information:
- Breathing airflow and breathing effort
- Blood oxygen level and pulse changes
- Heart rhythm or heart rate patterns
- Brain wave activity and sleep stages
- Eye movements and muscle activity
- Leg movements during sleep
- Snoring, body position and awakenings
- Events that interrupt stable sleep
The result is not based on one signal alone. Sleep specialists review the pattern across the night, including how often breathing events occur, whether oxygen levels drop, how sleep is fragmented, and whether the findings match the patient’s symptoms. A person who says they slept poorly in the lab may still provide enough useful data for interpretation, depending on how much sleep was recorded and what events occurred.
For patients, the most important point is that the study gives the physician objective information. Without testing, symptoms such as snoring, fatigue, insomnia, morning headache, and restless sleep can overlap with many possible causes. With testing, the care team can better determine whether a sleep-related breathing disorder, movement disorder, abnormal sleep pattern, or another issue should be addressed.
Sleep Problems and What Testing May Help Clarify
Sleep symptoms often overlap. Two patients may both say they are tired, but one may have breathing pauses, another may have insomnia, another may have restless legs, and another may have poor sleep because of pain, medication timing, anxiety, or shift work. The table below shows how testing may help organize the clinical picture.
| Patient concern | What the test may observe | Why the information matters |
|---|---|---|
| Loud snoring with pauses | Breathing interruptions, oxygen changes and arousals | Helps determine whether nighttime breathing is repeatedly disrupted |
| Morning headaches | Oxygen patterns, breathing changes and sleep fragmentation | May help connect symptoms with nighttime physiology |
| Daytime sleepiness | Sleep structure, awakenings and breathing-related events | Helps explain why hours in bed may not feel restorative |
| Frequent awakenings | Arousals, movement, breathing changes or other interruptions | May identify patterns the patient does not remember |
| Restless sleep or kicking | Leg movements and related awakenings | Helps evaluate whether movement is disrupting rest |
| Unrefreshing sleep with medical risks | Multiple sleep and body signals across the night | Supports a more complete discussion with the physician |
Overnight Lab Study vs Home Sleep Testing
Patients often ask whether they need to spend a night in a sleep lab or whether a home test is enough. The answer depends on the patient’s symptoms, medical history, suspected condition, insurance requirements, and the physician’s judgment. These tests are not identical, and choosing the right one matters.
An overnight lab study, also called polysomnography, is more comprehensive. It records multiple body signals while trained staff monitor the study. This may be useful when the physician needs detailed sleep staging, movement information, oxygen changes, breathing effort, heart rhythm data, or evaluation of more complex sleep concerns. The lab setting can also be appropriate when home testing may not provide enough information.
A home sleep test is usually more limited. It is often designed to evaluate suspected obstructive sleep apnea in selected patients. It may be more convenient because the patient sleeps in their own bed, but it may not record the same full range of information as an in-lab study. For example, some home tests do not measure sleep stages in the same way as a lab study, and they may be less suitable when symptoms suggest another sleep disorder or when significant medical conditions are present.
This is why patients should not choose testing based only on convenience. A home test that is easy to complete but not appropriate for the clinical question may lead to incomplete information. A lab study that collects more data may be better in some cases, but it may not be necessary for every patient. The physician’s role is to match the test to the question being asked.
| Setting | What it may be best for | Patient experience | Limitations |
|---|---|---|---|
| Overnight facility-based testing | More detailed evaluation of breathing, sleep stages, movement and related signals | The patient sleeps in a monitored room with sensors placed by trained staff | Sleeping away from home may feel unfamiliar for some patients |
| Home-based testing | Selected cases where nighttime breathing problems are the main concern | The patient uses equipment at home after receiving instructions | It may collect fewer signals and may not answer every sleep-related question |
| Follow-up testing | Situations where treatment response or changing symptoms need reassessment | The format depends on the clinical reason for repeating the test | Not always needed unless the physician has a specific reason |
A normal or unclear result should also be interpreted carefully. If symptoms remain significant, the physician may review whether the test matched the patient’s risk, whether enough data were collected, whether another condition should be considered, or whether additional evaluation is needed. Sleep medicine is not only about one report; it is about connecting the report to the patient’s real symptoms and health history.
How to Prepare Before Your Appointment
Preparation for an overnight sleep test is usually simple, but it matters. The goal is not to create an artificial perfect night. The goal is to help the sleep team collect useful information while avoiding avoidable factors that could disrupt the study or interfere with sensor placement. Patients should follow the instructions from their own sleep center because preparation may vary depending on the test type, medical history, medications, and facility protocol.
Before the appointment, the patient should ask whether any medications should be taken as usual or discussed in advance. Some medications can affect sleep architecture, breathing, alertness, muscle activity, or daytime sleepiness. Patients should not stop prescribed medication on their own before the test unless the ordering clinician gives specific instructions. A complete medication and supplement list can help the care team interpret results more accurately.
Many sleep centers advise patients to avoid caffeine and alcohol later in the day before testing because both can affect sleep quality and nighttime patterns. Caffeine may make it harder to fall asleep, while alcohol can alter breathing and sleep structure. Patients who drink alcohol regularly should not abruptly change habits without medical guidance; they should ask the clinician how to prepare safely.
Skin preparation can also matter. Lotions, oils, gels, heavy hair products, colognes, or makeup may interfere with sensors and adhesive. Patients are often advised to shower or bathe before arriving and to keep skin and hair clean and free of products. This is not about appearance; it helps the technologist attach sensors securely so the study can collect stable data.
Patients should also ask what to bring. An overnight study usually feels easier when the patient brings comfortable sleepwear, toiletries, reading glasses, a phone charger, necessary medications, and any personal items allowed by the facility. If the patient uses a nighttime device or has special needs, the sleep lab should be informed in advance.
Practical Preparation Checklist
A focused checklist can reduce stress before the test and help the night go more smoothly:
- Follow the instructions provided by the sleep center
- Ask whether medications should be taken as usual
- Avoid late caffeine or alcohol if instructed
- Arrive with clean skin and hair without heavy products
- Bring comfortable sleepwear and basic overnight items
- Bring a medication list and relevant medical information
- Tell the care team about special needs or mobility concerns
- Ask when and how results will be reviewed
Patients who worry they will not sleep in the lab should mention that concern before the test. It is common to sleep differently in a monitored setting. The room, sensors, and awareness of being tested can make the night feel unusual. In many cases, the study can still provide useful information even if the patient does not sleep exactly as they would at home.
It is also reasonable to ask about arrival time, parking, check-in process, room setup, bathroom access, and whether a family member can accompany the patient when needed. These practical details can reduce anxiety and make the test feel less unfamiliar.
What Happens When You Arrive at the Sleep Lab
When a patient arrives at the sleep lab, the first step is usually check-in and review of basic information. The team may confirm the patient’s identity, physician order, medications, symptoms, usual sleep schedule, and any special instructions. This helps make sure the correct test is performed and that the sleep technologist understands the clinical reason for the study.
The patient is then shown to a private or semi-private sleep room depending on the facility. Sleep labs are designed to support overnight monitoring, but the room is usually made to feel more comfortable than a typical exam room. The patient changes into sleepwear, prepares for bed, and the technologist begins placing sensors.
Sensor placement may take time. Electrodes may be attached to the scalp, face, chin, chest, abdomen, legs, and finger, depending on the study. Belts may be placed around the chest and abdomen to measure breathing effort. A small sensor near the nose or mouth may measure airflow. A finger sensor may measure oxygen level and pulse. These devices are connected to recording equipment so the technologist can monitor the study from another room.
The sensors may feel unfamiliar, but they should not be painful. Patients can usually move in bed, change position, and use the bathroom if needed. If a wire becomes loose or the patient needs assistance, the technologist can help. Most sleep labs have a way for the patient to communicate with staff during the night.
Before the study begins, the technologist may ask the patient to perform simple movements or breathing actions while awake. This helps confirm that the sensors are recording properly. The patient may be asked to move the eyes, clench the teeth, breathe in a certain way, or move the legs. These steps are part of calibration and help improve the quality of the recording.
Once the setup is complete, the lights are turned off and the patient tries to sleep. The technologist monitors signals during the night but does not usually enter the room unless a sensor needs adjustment, assistance is requested, or the study protocol requires it. The patient does not need to “perform” sleep. The goal is simply to rest as naturally as possible under the circumstances.
Some studies may involve treatment adjustment during the night if the test is designed that way. For example, certain patients being evaluated for sleep-related breathing problems may have positive airway pressure introduced or adjusted during a titration study. This depends on the physician order and the protocol of the sleep center. Not every diagnostic study includes treatment during the same night.
In the morning, the technologist removes the sensors. The patient may be able to leave shortly afterward unless the facility has additional instructions. The technologist usually does not provide a full diagnosis immediately because the recorded data must be reviewed and interpreted by qualified professionals. Patients should ask when the final report will be available and who will explain the results.
What Your Results Can Tell Your Physician
After the study, the recorded signals are reviewed to identify sleep stages, breathing events, oxygen changes, awakenings, movements, heart rate patterns, and other clinically relevant findings. The report helps the physician connect nighttime data with the patient’s symptoms and medical history. It does not replace the clinical conversation; it gives that conversation stronger evidence.
For suspected obstructive sleep apnea, one of the key questions is whether breathing repeatedly slows or stops during sleep. The report may describe how often these events occurred, whether they were linked with oxygen drops or arousals, and whether they were worse in certain positions or sleep stages. This information can help guide treatment discussions.
Results may also show whether the patient spent enough time in different sleep stages, whether sleep was fragmented, whether leg movements were frequent, or whether another pattern needs further evaluation. Some findings are clear, while others require careful interpretation. A patient should avoid trying to interpret the report alone without clinical context.
For patients with high blood pressure, heart rhythm concerns, diabetes risk, obesity, daytime sleepiness, or morning headaches, the sleep report may become part of a broader health plan. If disrupted breathing or poor sleep quality is identified, treatment may support better energy, safer daytime functioning, and more coordinated chronic disease care. Patients focused on prevention can also review lifestyle habits that support heart health.
Sometimes a sleep study does not show the suspected problem. This does not mean the patient’s symptoms are imaginary. It may mean that another cause should be considered, that the test did not capture a typical night, that insomnia or schedule issues are playing a larger role, or that follow-up evaluation is needed. The physician can help decide whether additional testing, behavioral sleep treatment, medication review, or another specialty evaluation is appropriate.
Patients should ask the physician to explain the result in plain language. Useful questions include what diagnosis was found, how severe it is, what treatment options are available, whether follow-up is needed, and what symptoms should improve if treatment works. A clear explanation helps patients move from diagnosis to action rather than leaving the report as a confusing set of numbers.
What Happens After Diagnosis
The next step after a sleep diagnosis depends on the condition found, the severity of the findings, the patient’s symptoms, and other medical risks. The goal is not simply to label the problem, but to choose a treatment or follow-up plan that fits the patient’s life and health needs.
For obstructive sleep apnea, treatment options may include positive airway pressure therapy, oral appliances in selected cases, weight-related counseling when appropriate, positional strategies, management of nasal obstruction, or referral to another specialist. The right plan depends on the patient’s anatomy, severity, comfort, insurance coverage, medical history, and ability to use the treatment consistently.
If insomnia is the major concern, treatment may focus on behavioral strategies, sleep schedule consistency, medication review, anxiety or mood assessment, pain control, caffeine timing, or referral for cognitive behavioral therapy for insomnia when available. A sleep study may help rule in or rule out certain contributing problems, but insomnia often requires a plan beyond one night of testing.
If movement-related sleep disruption is found, the physician may review medications, iron status when appropriate, neurologic symptoms, or other contributing factors. If unusual behaviors during sleep are reported, additional evaluation may be needed to understand whether the episodes are related to sleep stage, medication effects, neurologic conditions, stress, or another cause.
Treatment follow-up is important because sleep therapy only helps when it is used effectively. A patient may need mask adjustments, pressure changes, comfort troubleshooting, education, repeat assessment, or help with side effects. Difficulty using treatment should be discussed early rather than treated as failure.
Follow-up also helps connect sleep care to the rest of the patient’s health. If the patient has high blood pressure, daytime sleepiness, mood symptoms, weight concerns, or heart risk factors, the sleep diagnosis may become part of a broader care plan. Primary care can help coordinate this process, especially when several conditions overlap.
How Sleep Testing Fits Into Long-Term Health Care
Sleep testing is often most useful when it is connected to the rest of the patient’s medical care. Poor sleep can affect daytime safety, mood, memory, work performance, blood pressure, weight management, and chronic disease control. At the same time, medical conditions, medications, pain, stress, hormonal changes, and breathing problems can affect sleep. This two-way relationship is why sleep should not be treated as a separate lifestyle issue when symptoms are persistent.
For patients with suspected sleep apnea, the goal of sleep apnea testing is to determine whether breathing interruptions are occurring often enough to affect health and daily functioning. If testing confirms a clinically significant problem, the physician can discuss treatment options and follow-up. If testing does not confirm the suspected condition, the care team can look for other explanations, such as insomnia, medication effects, pain, mood disorders, schedule disruption, or another medical concern.
A sleep disorder clinic can also help patients who have tried to manage symptoms alone without success. Many people buy pillows, change mattresses, use phone apps, take supplements, or adjust bedtime routines before seeking medical care. These steps may help some patients, but they may not address breathing interruptions, oxygen changes, movement-related disruption, or other problems that require a medical plan.
Sleep information may be especially important for patients with cardiovascular risk factors. If a patient has high blood pressure, heart rhythm concerns, obesity, diabetes risk, or daytime sleepiness, the physician may use sleep results as part of a broader prevention strategy. This does not mean sleep testing replaces primary care, heart care, nutrition counseling, medication review, or regular monitoring. It means the sleep report can give the care team another piece of objective information.
Patients should also understand that treatment response may take time. If positive airway pressure therapy, an oral appliance, behavioral treatment, or another approach is recommended, the first few weeks may require adjustment. Comfort, mask fit, dryness, pressure sensation, schedule consistency, and anxiety about equipment can all affect adherence. Early communication with the care team can prevent small barriers from becoming reasons to abandon treatment.
The most useful sleep care does not stop at diagnosis; it connects test results, symptoms, treatment comfort, follow-up data, and the patient’s broader health goals.
Questions to Ask Before and After Your Study
Patients often feel more comfortable when they know what to ask before the appointment and during the follow-up visit. A sleep test can generate a detailed report, but the patient needs clear explanations, not just numbers. Good questions help turn the study into a practical care plan.
Before the Test
Before the study, patients should ask what type of test is being ordered, why that test was chosen, whether it will be done at home or in a lab, how to prepare, what to bring, and whether medications should be taken as usual. Patients should also ask how long the test will take and when results are expected.
After the Test
After the report is reviewed, patients should ask what the results mean, whether a diagnosis was made, how severe the findings are, what treatment options exist, and what follow-up is needed. If treatment is recommended, the patient should ask what improvement to expect, how success will be measured, and who to contact if the treatment is uncomfortable or difficult to use.
When Symptoms Continue
If symptoms continue after testing or treatment, patients should not assume that nothing can be done. Persistent fatigue, insomnia, morning headaches, snoring, nighttime awakenings, mood changes, or poor concentration may need another review. The physician may reconsider the diagnosis, adjust treatment, evaluate medication effects, review other medical conditions, or recommend another type of care.
Common Myths About Sleep Studies
Misunderstandings about sleep testing can delay care. Some patients avoid evaluation because they believe the test will be painful, impossible to sleep through, or only useful for people with severe symptoms. In reality, sleep testing is designed to collect medical information while the patient rests, and the level of testing can be matched to the clinical question.
One common myth is that a patient must sleep perfectly for the study to work. Most patients do not sleep exactly as they do at home, especially during an overnight lab study. The sensors, room, and awareness of testing can feel unusual. However, many studies still collect enough useful data for interpretation. If the night produces too little information, the physician can explain whether repeating or changing the testing approach is needed.
Another myth is that snoring alone is harmless. Snoring can be simple and may not always mean a medical disorder is present. However, loud snoring with pauses in breathing, gasping, choking, morning headaches, high blood pressure, or daytime sleepiness should be discussed with a clinician. The concern is not the sound itself, but whether breathing and oxygen levels are being disrupted during sleep.
Some patients also assume that a home test is always better because it is more convenient. Convenience matters, but it is not the only factor. A home test may be appropriate for selected patients, while an overnight lab study may be more useful when the physician needs more complete data or when symptoms are complex. The best test is the one that answers the medical question accurately enough to guide care.
Another misunderstanding is that diagnosis automatically means lifelong complicated treatment. Treatment depends on the condition, severity, symptoms, anatomy, patient preference, and medical history. Some patients need positive airway pressure therapy. Others may need behavioral sleep treatment, dental appliance evaluation, positional strategies, medication review, weight-related counseling, or specialist referral. The plan should be individualized.
Medical Disclaimer
This article is for educational purposes only and does not replace professional medical advice, diagnosis, or treatment. If you have severe shortness of breath, chest pain, fainting, confusion, stroke-like symptoms, dangerously high blood pressure, or another urgent concern, seek emergency medical care immediately.
Author
By Dr. Cody R. Christensen, M.D. He practices at Sweetwater Medical Center, where he integrates pharmacologic treatment with lifestyle medicine and psychotherapy to support lasting patient wellness.
Medically Reviewed: by Clinical Pharmacy Board
Last Updated: 08.06.2026
FAQ
Is a sleep study painful?
No. The sensors may feel unfamiliar, but they are used for recording signals and should not be painful. Patients can usually ask the technologist for help if something feels uncomfortable during the night.
Can I sleep normally with sensors attached?
Many patients sleep differently during the test because the setting is unfamiliar. Even so, the study may still collect enough useful information for interpretation.
How long does it take to receive results?
The timing depends on the sleep center and the type of study. The recorded data usually need professional review before the physician explains the results and next steps.
Is home testing the same as an overnight lab test?
No. Home testing is usually more limited and is often used for selected patients when nighttime breathing problems are the main concern. An overnight lab study can collect a broader range of sleep and body signals.
Can untreated sleep apnea affect blood pressure?
Sleep apnea can be associated with cardiovascular strain and may contribute to difficult-to-control blood pressure in some patients. A clinician can decide whether sleep evaluation should be part of the patient’s broader health plan.