
Why Hospital Care Is a Team Effort
A hospital stay can feel overwhelming because patients often meet many professionals in a short period of time. One person checks vital signs, another brings medication, another asks about pain, another takes blood, another explains a test, and another discusses discharge. Behind all of these interactions is a coordinated sweetwatermedical hospital care team working to evaluate the patient, monitor changes, provide treatment, reduce risk, and prepare for recovery after leaving the hospital.
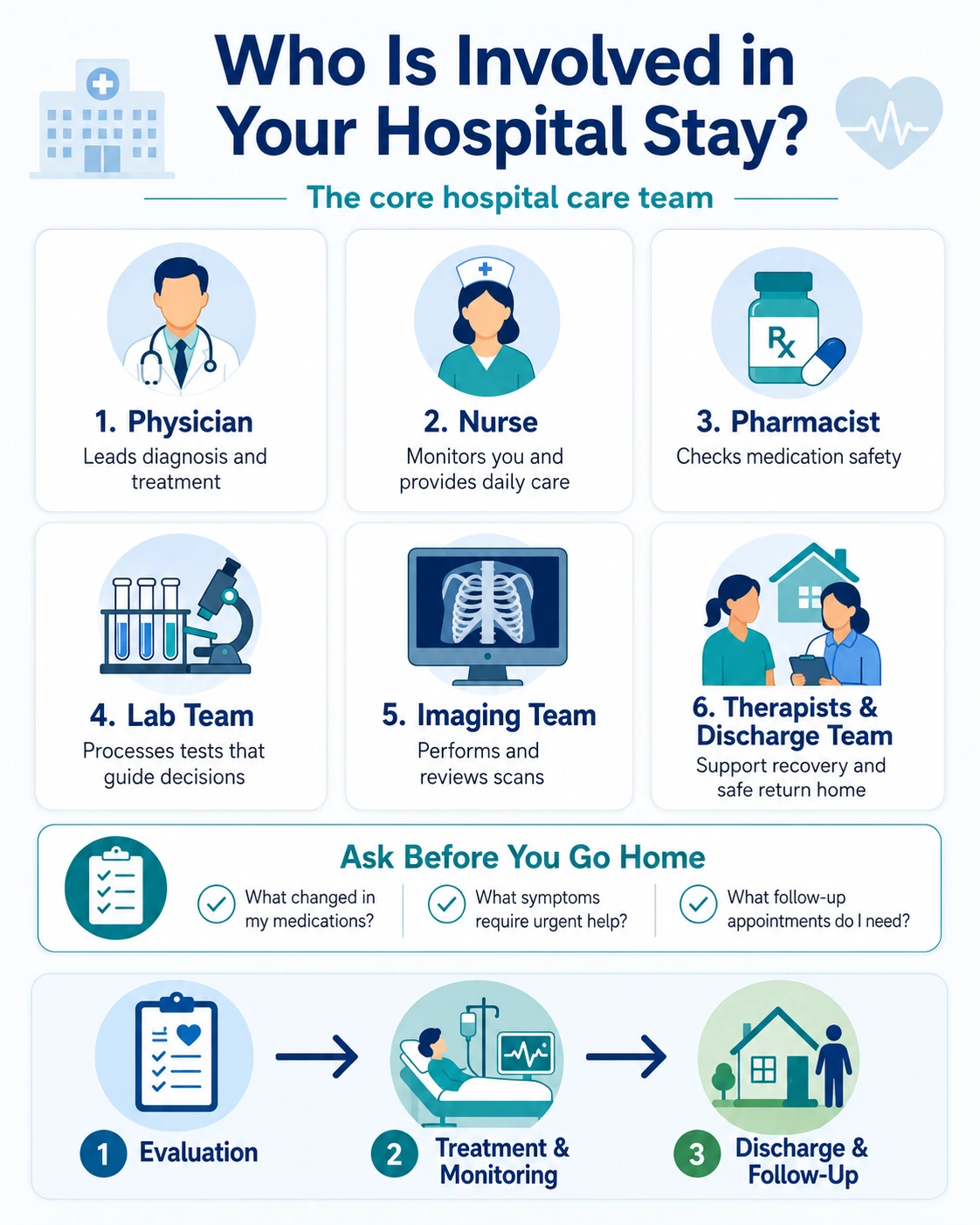
Many patients assume hospital care is mainly directed by one physician. The physician’s role is central, but hospital care depends on more than one person. Doctors, nurses, pharmacists, laboratory professionals, imaging specialists, respiratory therapists, rehabilitation teams, social workers, care coordinators, dietitians, and support staff may all contribute depending on the patient’s condition. Some team members work at the bedside. Others work behind the scenes, but their decisions and tasks still affect the patient’s care.
The safest hospital care usually comes from coordination: each professional contributes a different type of expertise, and the patient benefits when those roles connect clearly.
A patient admitted for chest pain, infection, surgery, breathing problems, stroke symptoms, injury, uncontrolled blood pressure, dehydration, or worsening chronic disease may need several departments involved. Laboratory testing may help evaluate infection, anemia, kidney function, medication safety, or inflammation. Imaging may help clarify injury, internal disease, or complications. Pharmacy review may help reduce medication interactions. Nursing observation may detect small changes before they become major concerns.
The care team also changes over time. The people involved during admission may not be the same as those involved during recovery or discharge. A patient may first meet emergency clinicians, then hospital physicians, nurses, laboratory staff, imaging technologists, therapists, and discharge planners. This can feel confusing unless patients understand the purpose of each role.
Communication is often the most important part of the experience. A patient may hear medical information from several people and wonder who is responsible for the final plan. In most cases, the attending physician or primary hospital physician coordinates major treatment decisions, while nurses, specialists, pharmacists, therapists, and other professionals contribute specific expertise. Patients should feel comfortable asking who is leading the plan and who can answer different types of questions.
Laboratory work is one example of behind-the-scenes teamwork. Patients may only see the blood draw, but the sample then moves through processing, analysis, quality checks, and reporting before the physician uses the result. A separate guide on the laboratory team behind faster diagnosis explains that process in more detail.
Imaging is another example. A patient may interact with an imaging technologist during an X-ray, CT, MRI, ultrasound, or mammogram, but the final interpretation usually comes from a radiologist and then returns to the treating physician. Patients who want to understand this part of the process can review how imaging helps physicians clarify findings.
The purpose of this guide is to help patients and families understand who may be involved during a hospital stay, what each role usually contributes, and which questions to ask before discharge. The exact team depends on the hospital, department, diagnosis, staffing model, and patient needs, but the principles of coordinated care remain the same.
The Physician’s Role During Your Stay
Physicians are responsible for evaluating the patient’s condition, forming a diagnosis or working diagnosis, ordering tests, prescribing treatment, consulting specialists when needed, and deciding whether the patient is safe for discharge. In a hospital setting, this may involve an attending physician, hospitalist, surgeon, emergency physician, specialist, resident physician, or advanced practice clinician depending on the care model.
The attending physician or lead hospital clinician usually coordinates the overall plan. This person reviews the patient’s symptoms, medical history, exam findings, medication list, test results, imaging, and response to treatment. They decide whether more testing is needed, whether medications should change, whether a specialist should be involved, and what must happen before the patient can leave the hospital safely.
Specialists may become involved when the patient’s condition requires focused expertise. A cardiologist may help with heart rhythm, chest pain, heart failure, or blood pressure concerns. A neurologist may evaluate stroke-like symptoms, seizures, weakness, or complex headaches. A pulmonologist may help with severe breathing problems. A surgeon may evaluate injuries, abdominal emergencies, wounds, or operative needs. The specialist provides targeted recommendations, while the primary hospital team helps integrate those recommendations into the full care plan.
Physicians also communicate risk and uncertainty. Not every hospital diagnosis is clear on the first day. A patient may be admitted with a set of symptoms while the team rules out several possibilities. The physician’s job is to explain what is known, what is still being evaluated, what tests are pending, and what signs would change the plan. Patients should ask for clarification when the plan feels unclear.
Another major responsibility is medication decision-making. The physician decides which home medications should continue, which should pause, which new medications are needed, and which doses should change because of kidney function, blood pressure, infection, surgery, pain, bleeding risk, or other factors. These decisions are often made with input from nurses, pharmacists, laboratory results, and specialists.
Before discharge, the physician determines whether the patient is medically stable, whether symptoms have improved enough, whether test results are reassuring or require follow-up, and whether a safe plan exists outside the hospital. Discharge does not always mean every problem is fully solved. It usually means the patient no longer needs hospital-level care and can continue recovery with instructions, medication, follow-up, and warning signs.
Nurses: The Team Members Patients See Most Often
Nurses are often the professionals patients interact with most during a hospital stay. They monitor symptoms, check vital signs, administer medications, assess pain, watch for changes, communicate with physicians, educate patients, coordinate daily care, and help patients understand what is happening. Because nurses spend more time at the bedside, they often notice changes early.
A nurse may be the first person to recognize that a patient’s breathing has worsened, blood pressure has changed, pain is not controlled, confusion has developed, a medication side effect may be present, or a wound looks different. These observations can trigger a physician reassessment, new orders, additional testing, medication adjustment, or escalation of care.
Nurses also help translate the care plan into daily actions. The physician may order medications, activity restrictions, diet changes, laboratory tests, imaging, wound care, or monitoring. Nurses help carry out these orders and explain what the patient should expect. They may also teach patients how to use equipment, track symptoms, prevent falls, manage pain, or prepare for discharge.
Medication administration is a major nursing responsibility. Nurses check the medication, dose, timing, route, patient identity, allergies, and sometimes relevant vital signs or lab results before giving a drug. If a medication seems unsafe or the patient reports a concern, the nurse can contact the physician or pharmacist for clarification.
Nurses also support patient safety. They help reduce fall risk, monitor for pressure injuries, prevent infection when possible, assess mobility, respond to alarms, and ensure that changes are communicated to the right professional. Patients should tell the nurse about new pain, dizziness, breathing difficulty, nausea, weakness, confusion, bleeding, allergic symptoms, or anything that feels different.
Families often ask nurses practical questions because they are accessible throughout the day. A nurse can usually explain the schedule of medications, tests, meals, mobility support, and routine monitoring. However, questions about diagnosis, prognosis, major treatment decisions, or discharge timing may need to be answered by the physician or lead clinician.
Who Does What During a Hospital Stay
The table below gives a general overview of common roles in hospital care. The exact team depends on the hospital, diagnosis, patient needs, staffing model, and whether the patient is in an emergency department, inpatient unit, intensive care unit, surgical unit, rehabilitation unit, or observation area.
| Team member | Main role | When patients may interact with them | Questions they may help answer |
|---|---|---|---|
| Physician or lead clinician | Directs diagnosis, treatment plan, testing and discharge decisions | During rounds, admission review, major updates or discharge planning | What is the diagnosis, what is the plan, and what must happen before discharge? |
| Nurse | Monitors condition, gives medications, assesses symptoms and coordinates daily care | Throughout the hospital stay | What is scheduled today, when are medications due, and what symptoms should be reported? |
| Pharmacist | Reviews medication safety, interactions, dosing and transitions of care | When medication review, counseling or discharge planning is needed | How should this medication be taken, and what side effects should be watched? |
| Laboratory professional | Processes and analyzes specimens used in diagnosis and monitoring | Usually behind the scenes, sometimes during collection | Most result questions should be directed to the clinician interpreting the report |
| Imaging technologist | Performs imaging exams ordered by the clinician | During X-ray, CT, MRI, ultrasound or other imaging procedures | How will the exam be performed, and what preparation is needed? |
| Radiologist | Interprets imaging and sends a report to the care team | Often behind the scenes unless direct consultation is needed | The ordering clinician usually explains how the report affects care |
| Therapist | Assesses mobility, strength, breathing, swallowing, function or recovery needs | During rehabilitation, post-surgery care or discharge planning | What activities are safe, and what support is needed after discharge? |
| Care coordinator or social worker | Helps organize discharge needs, services, equipment and community resources | When the patient needs support after leaving the hospital | What help is needed at home, and what follow-up has been arranged? |
Pharmacists, Lab Professionals and Imaging Specialists
Some of the most important members of the care team work partly or entirely behind the scenes. Patients may not always meet the pharmacist who reviews a medication list, the laboratory professional who processes a specimen, the radiologist who interprets a scan, or the imaging technologist who prepares the equipment. Still, these roles can strongly affect diagnosis, safety, treatment decisions, and discharge planning.
Hospital pharmacists help reduce medication-related risk. They may review drug interactions, allergies, kidney or liver dosing, duplicate therapies, anticoagulants, antibiotics, pain medications, insulin, high-risk drugs, and medications that should be restarted or stopped before discharge. This is especially important for patients who take several prescriptions, have chronic disease, are older, or are being treated by multiple specialists.
Pharmacists may also help with medication reconciliation. This means comparing the medications the patient was taking before admission with the medications ordered in the hospital and the medications planned after discharge. A medication that seems small can matter if the dose is wrong, if it interacts with another drug, or if the patient does not understand how to take it at home.
Laboratory professionals support diagnosis by processing and analyzing samples. A patient may only remember a blood draw, urine sample, or swab, but the result may influence antibiotic decisions, kidney monitoring, anemia evaluation, blood sugar control, infection assessment, medication safety, and cancer-related follow-up. The laboratory does not replace the physician’s judgment; it provides objective information the physician uses in context.
Pathology may also be involved when tissue or cells need review. A biopsy, surgical specimen, suspicious lesion, abnormal screening result, or fluid sample may require microscopic interpretation. This work can be essential in determining whether a finding is benign, inflammatory, infectious, precancerous, malignant, or unclear. Patients may never meet the pathologist, but the pathology report can guide major decisions.
Imaging specialists also play several roles. The technologist performs the exam, positions the patient, follows safety protocols, and helps obtain images of diagnostic quality. The radiologist interprets the images and sends a report to the treating clinician. The treating clinician then explains what the report means for the patient’s care plan. This chain is important because an image finding often needs clinical context before it can be understood correctly.
Patients should ask who will explain laboratory and imaging results. A technologist or laboratory professional may not be the right person to interpret findings at the bedside. In most cases, the ordering clinician or hospital physician should connect the result to the patient’s symptoms, diagnosis, and next steps.
Rehabilitation and Discharge Planning
Hospital care does not end when symptoms improve. Many patients need a plan for safe recovery after leaving the hospital. Rehabilitation specialists, discharge planners, social workers, nurses, physicians, pharmacists, and family caregivers may all be involved in deciding what support is needed at home or in another care setting.
Physical therapists may evaluate strength, balance, walking ability, fall risk, transfers, endurance, and whether the patient can safely move around after illness, injury, surgery, stroke, or prolonged bed rest. They may recommend exercises, walking support, assistive devices, home safety changes, outpatient therapy, inpatient rehabilitation, or skilled nursing care depending on the patient’s condition.
Occupational therapists may focus on daily function. This can include dressing, bathing, toileting, cooking, using stairs, managing fatigue, adapting the home, using equipment safely, and returning to daily routines. Their work is especially important when a patient’s illness affects independence.
Speech-language pathologists may become involved when swallowing, speech, cognition, or communication are affected. This can be relevant after stroke, neurologic illness, head injury, surgery, prolonged intubation, or other conditions. Their recommendations may affect diet, safety, communication strategies, and rehabilitation planning.
Respiratory therapists may help patients with breathing treatments, oxygen support, inhaler technique, airway clearance, ventilator support, sleep-related breathing support, or education about lung conditions. For patients admitted with pneumonia, COPD, asthma, heart failure, post-surgical breathing concerns, or oxygen needs, this role can be central to recovery.
Discharge planning helps prepare the next phase of care. A patient may need home health services, medical equipment, wound care, oxygen, therapy, transportation, medication access, specialist follow-up, primary care follow-up, or instructions for warning symptoms. A care coordinator or social worker may help organize these needs when the situation is complex.
Patients should not wait until the final hour to raise concerns about going home. If they live alone, have stairs, cannot afford medications, lack transportation, feel unsafe, do not understand instructions, or need help with daily tasks, the team should know early. A safe discharge plan depends on honest information about the patient’s real home situation.
What Patients and Families Can Ask the Care Team
Patients and families often feel more confident when they know what to ask. Hospital days can be busy, and information may come quickly. Writing down questions can help the patient understand the plan, avoid missed details, and prepare for discharge.
Questions That Can Clarify the Care Plan
The following questions can help patients and families understand what is happening during the hospital stay:
- What diagnosis is being considered right now?
- What test results are still pending?
- What medications were started, stopped or changed?
- What symptoms should be reported immediately?
- What needs to happen before discharge?
- Who will explain lab and imaging results?
- What follow-up appointments are needed after discharge?
- Who should be contacted if symptoms return at home?
Families can also ask how to support the patient safely. This may include helping with medication schedules, transportation, wound care, mobility, meals, follow-up visits, symptom monitoring, or communication with the clinic. The care team can only plan realistically when they understand what support is available.
Patients should also ask for explanations in plain language. Medical terms can be confusing, especially when several professionals use different words for the same problem. It is appropriate to ask, “What does that mean for me?” or “What is the next step?” Clear communication is part of safe care.
Behind-the-Scenes Interview Section
The section below can be used as an interview template for the hospital team. Once staff responses are collected, each answer can be edited for clarity while preserving the meaning of the original response.
Interview Questions for the Care Team
These questions can help create a human, trustworthy section inside the article:
- What do patients often misunderstand about your role?
- What helps your team work faster and safer?
- What should patients always tell you during a hospital stay?
- What makes discharge planning smoother?
- What do you wish families knew before taking a patient home?
- How does your work connect with physicians, nurses and other departments?
Photographs can also improve trust when used responsibly. The strongest format is not a stock image of a hospital hallway, but real images of the care team, laboratory, nursing station, rehabilitation space, pharmacy workflow, or imaging department, with patient privacy fully protected. Captions should identify roles clearly and avoid making medical claims that cannot be verified.
If the center does not yet have staff quotes, this section can remain as an editorial note or be replaced with a general explanation of team-based care. The key rule is accuracy: do not attribute words to staff members unless they actually said them.
How Follow-Up Care Continues After Discharge
Leaving the hospital does not always mean care is finished. In many cases, discharge is the transition from hospital-level monitoring to recovery at home, outpatient follow-up, rehabilitation, or specialist care. The patient should leave with a clear plan that explains medications, warning symptoms, activity limits, diet instructions, wound care, test follow-up, and the next appointments.
Primary care often becomes important after discharge because it helps connect the hospital stay to long-term health. A patient may need blood pressure follow-up, medication review, lab monitoring, imaging follow-up, sleep evaluation, chronic disease management, or preventive care after the acute problem improves. Patients can review follow-up visits that support long-term recovery to understand why continuity matters.
Medication changes are one of the most important parts of discharge. A patient may leave with new prescriptions, stopped medications, temporary medications, changed doses, or instructions to restart a medication later. Confusion at this stage can lead to missed doses, duplicate therapy, side effects, or readmission. Patients should ask the care team to explain which medications to take, when to take them, which ones were stopped, and why.
Pending results also need attention. Some laboratory, pathology, culture, or imaging results may not be finalized before the patient leaves. The discharge plan should say who will review those results and who will contact the patient if follow-up is needed. Patients should not assume that no news always means no issue. If a result is expected and not received, the patient should contact the care team.
Rehabilitation may continue after the hospital stay. Depending on the condition, a patient may need home exercises, outpatient physical therapy, occupational therapy, speech therapy, cardiac rehabilitation, pulmonary rehabilitation, or another recovery program. Follow-up care helps prevent avoidable complications and supports a safer return to normal activity.
Hospitalization can also be a turning point for prevention. A patient admitted with chest pain, infection, uncontrolled blood pressure, fall injury, breathing problems, or dehydration may need more than short-term treatment. The event may reveal a need to address long-term habits, home safety, medication management, sleep, nutrition, or cardiovascular risk. A broader prevention guide on heart-healthy habits after a medical visit can support that next step.
How Patients Can Participate in Safer Team-Based Care
Patients and families are not expected to manage the hospital stay alone, but they can support safer care by sharing accurate information and asking clear questions. The care team needs to know what medications the patient takes at home, what allergies are present, what symptoms are new, what changed before admission, and what support exists after discharge.
Patients should speak up when something feels different. New pain, worsening shortness of breath, dizziness, confusion, weakness, bleeding, rash, nausea, swelling, medication side effects, or difficulty walking should be reported promptly. Small changes can be clinically important, especially for older adults, patients after surgery, and those with heart, lung, kidney, neurologic, or immune-related conditions.
Families can help by observing patterns the patient may not notice. A family member may see confusion, weakness, breathing changes, poor appetite, sleepiness, or mobility problems before the patient reports them. They can also help remember instructions, medication changes, follow-up dates, and warning signs.
Patients should ask who to contact for different concerns. During the hospital stay, the nurse may be the best first contact for immediate bedside concerns. The physician may answer questions about diagnosis and major treatment decisions. The pharmacist may help clarify medication issues. The therapist may explain mobility and activity safety. The discharge planner may help with home services and equipment.
It is also reasonable to ask for information to be repeated. Hospital stays are stressful, and patients may be tired, medicated, anxious, or in pain. Written instructions, medication lists, follow-up appointments, and plain-language explanations can reduce confusion. A patient should not leave without understanding the next step.
Why Team-Based Care Builds Patient Trust
Trust is not built only by medical technology or hospital buildings. It is built when patients see that professionals communicate, listen, explain, and coordinate. A patient may not understand every test result or treatment decision, but they can often sense whether the team is organized and whether their concerns are being heard.
Team-based care also helps reduce blind spots. A physician may focus on diagnosis and treatment. A nurse may notice changes at the bedside. A pharmacist may identify a medication risk. A laboratory professional may flag an urgent result. An imaging specialist may clarify an internal finding. A therapist may identify that the patient cannot safely return home without support. Each role adds a different layer of safety.
The phrase inpatient care team describes more than job titles. It describes a system of shared responsibility. The patient’s experience improves when team members understand their roles, communicate clearly, and connect their work to the patient’s goals.
For the medical center, showing this team clearly can also strengthen credibility. Real staff photos, accurate role descriptions, department explanations, and verified quotes can help patients understand that care is delivered by people, not just processes. This is especially useful for patients who feel anxious about hospitalization or who have never been admitted before.
However, trust should not be built on exaggerated claims. The article should not promise perfect outcomes, instant answers, or a specific result from hospitalization. It should show the real strength of the center: coordinated professionals, diagnostic support, clear communication, and a plan that continues after discharge.
Medical Disclaimer
This article is for educational purposes only and does not replace professional medical advice, diagnosis, or treatment. Hospital care teams and roles vary by facility, department, diagnosis, and patient needs; ask your care team who is responsible for your treatment plan and follow-up instructions.
Author
By Dr. Cody R. Christensen, M.D. He practices at Sweetwater Medical Center, where he integrates pharmacologic treatment with lifestyle medicine and psychotherapy to support lasting patient wellness.
Medically Reviewed: by Clinical Pharmacy Board
Last Updated: 08.06.2026
FAQ
Who is in charge of my hospital care?
The attending physician or lead hospital clinician usually coordinates the main care plan. Specialists, nurses, pharmacists, therapists, laboratory teams, imaging teams, and discharge planners may contribute depending on your condition.
Why do I see different doctors during one stay?
Hospital care often involves several clinicians because different problems may require different expertise. One physician may coordinate the plan while specialists provide focused recommendations.
Can I ask nurses about my treatment plan?
Yes. Nurses can often explain daily care, medications, monitoring, symptoms to report, and what is scheduled. Questions about diagnosis, prognosis, or major treatment decisions may need the physician or lead clinician.
What does a hospital pharmacist do?
A hospital pharmacist may review medication safety, interactions, allergies, dosing, and discharge medication changes. This can reduce medication-related risks during and after the hospital stay.
What should I ask before discharge?
Ask which medications changed, what symptoms require urgent care, which results are pending, what follow-up appointments are needed, and who to contact if problems return at home.